


Neuroplasticity in Tendinopathy
by Martin Krause
A multitude of contributing factors to altered motor control must be addressed when treating tendon dysfunction. What we have failed to consider in the past when dealing with chronic or recurrent tendon issues are motor control problems encompassing corticospinal control of excitation and inhibition as well as belief systems about pain and contextual factors related to imaging.
Research by Ebonie Rio et al (2015) (BJSM Sept 25, 10.1136/bjsports-2015-095215) suggest that the pain state sets up an adaptive pathway whereby the ipsilateral kinetic chain is directly inhibited by reflexogenic pathways, as well as being inhibited by contralateral hemispheric activity. Simultaneously excitation is enhanced in the opposite limb as well as in antagonists...at least in the case of enhanced excitation of the hamstrings in quadricep tendinopathy. If this is true, then so much for training the contralateral limb for 'cross training' purposes! This may also explain why a lot of people seem to have "all their injuries on the same side" (of the body). Furthermore, they recommend enhancing corticospinal drive through the use of 30-60 second isometric holds at 70-80% MVC to load the muscle whilst using isokinetics to load the tendon. Moreover, they recommend the use of a metronome at 60bpm (stages 1 and 2) with a count of 3 up, 2 down for quads, and 2 up, 3 down for calf isokinetics to optimally engage corticospinal drive through the visual and auditory stimuli (also shown by Kohei et al 2012 {Int J Rehab Res, 35, 1, 82-84} for motor imagery and M1 stimulation) .....read more
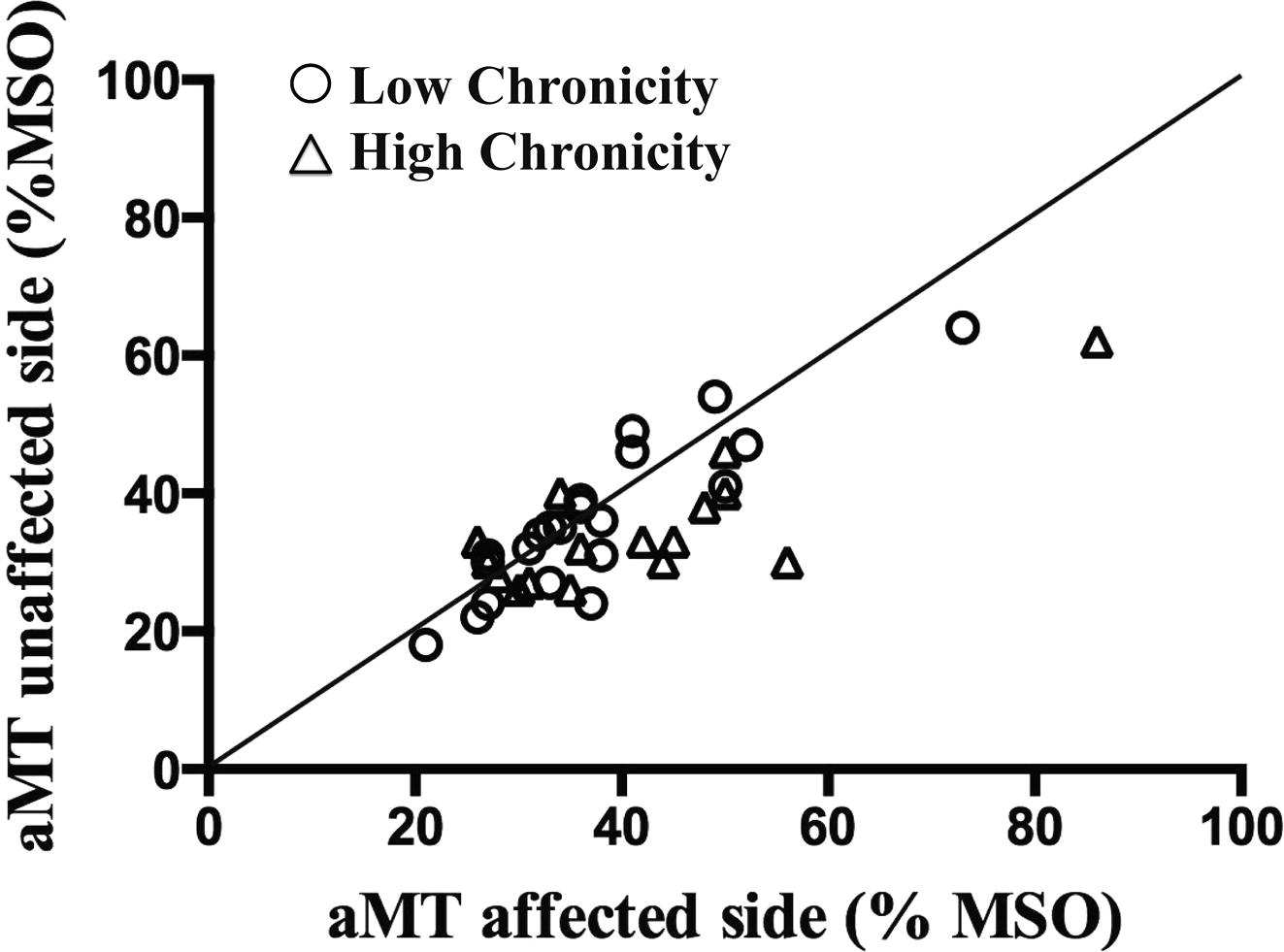
Cortical mapping of infraspinatus muscle in chronic shoulder pain demonstrating higher motor thresholds (aMT= activation MT) and hence reduced excitability on the affected side (39 vs 35) (Ngomo et al 2015 Clinical Neurophysiol, 126, 2, 365-371)
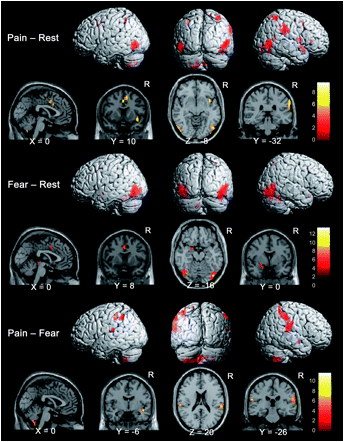
Cortical mapping of pain and fear. Lots of overlap suggesting that taking away the fear from the pain with clear clinical explanations and a focused goal directed program using specific functional outcomes is important.
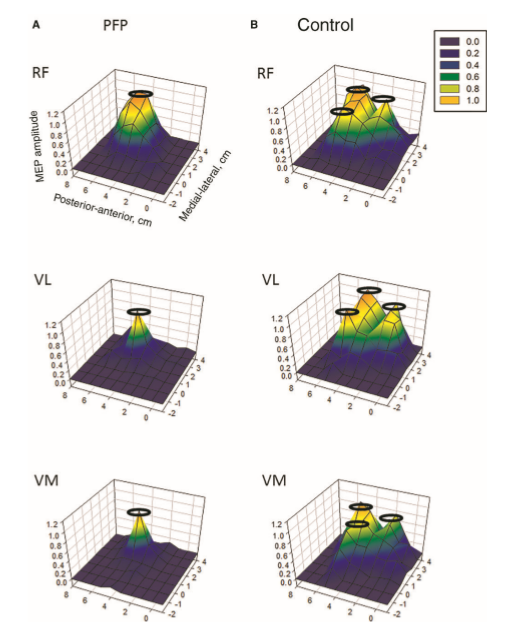
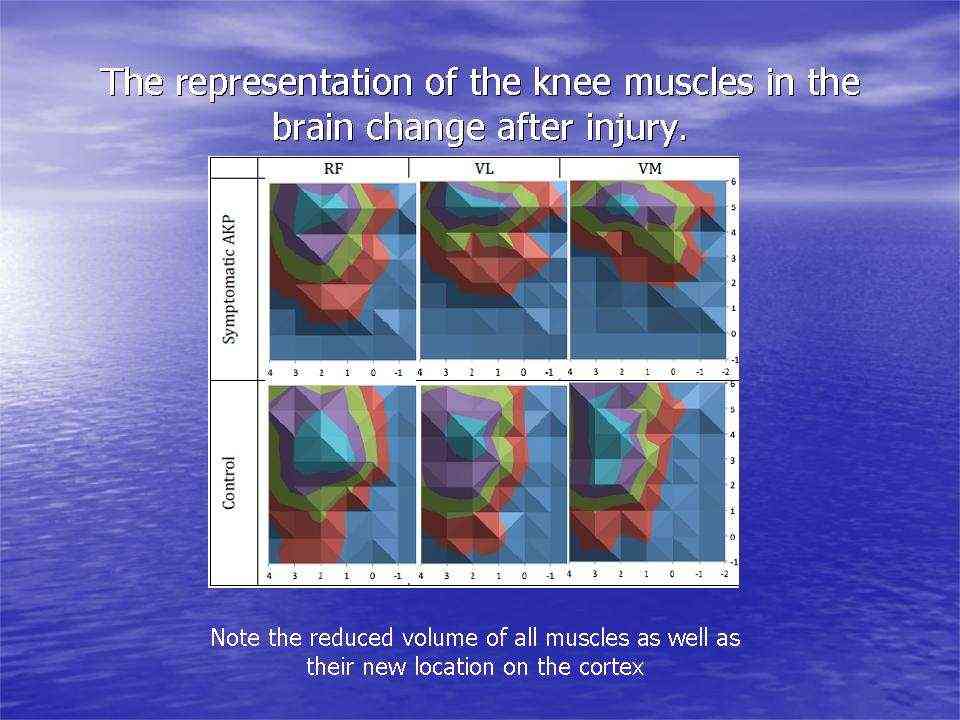
Individuals with patellofemoral pain (PFP) had reduced map volumes and an anterior shift in the M1 representations, greater overlap of the M1 representation and a reduction in cortical peaks across all three quadriceps (RF, VL, VMO) muscles compared with controls.(Te et al 2017 Pain Medicine, pnx036, https://doi.org/10.1093/pm/pnx036)
Uploaded : 18 October 2017
